Dermatology Emollient's and Topical Steroids
Online recording exploring the use of emollients and topical steroid use for skin conditions in primary care.
Last updated
Thu, 29-Aug-2024
Online recording exploring the use of emollients and topical steroid use for skin conditions in primary care.
Last updated
Thu, 29-Aug-2024
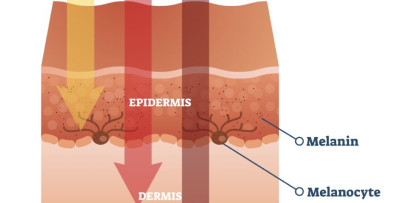
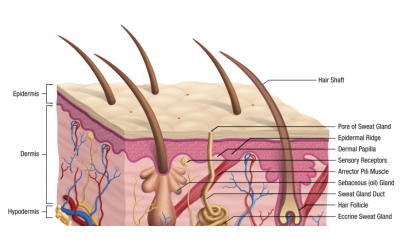
Emollients are used for the first-line treatment of a wide variety of dry or eczematous skin disorders. Since their soothing and hydrating properties are short-lived, they require frequent liberal application, especially after bathing, with continued use after improvement occurs. A wide variety of preparations are available, with choice guided by the severity of the condition, site of application and patient preference.
Topical steroids are used intermittently for acute exacerbations of inflammatory skin disorders where other measures such as emollients are ineffective. Steroids suppress the inflammatory reaction during use; they are not curative and on discontinuation a rebound exacerbation of the condition may occur. Again, a wide variety of preparations are available, with choice guided by the severity of the condition, site of application and age of the patient. Topical steroids are associated with adverse effects – skin thinning, spreading of untreated infection, striae, acne and mild depigmentation. To minimise potential adverse effects, the least potent formulation which is fully effective should be used, it should be spread thinly on the affected areas only (measured in terms of fingertip units) application should not be more frequent than twice daily.
There appears to be no real consensus on the timing of the application of emollients and topical steroids in conjunction with each other. This E-learning audio recording explores use of emollients and topical steroids by a consultant dermatologist who works in primary care


+VAT